Introduction
Physical therapy in Baton Rouge for Knee
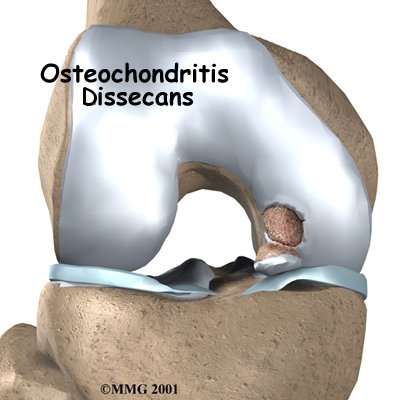
Welcome to Peak Performance Physical Therapy's patient resource about Osteochondritis Dissecans of the Knee.
Osteochondritis dissecans (OCD) is a problem that affects the knee, mostly at the end of the big bone of the thigh (the femur). A joint surface damaged by OCD doesn't heal naturally. Even with surgery, OCD usually leads to future joint problems, including degenerative arthritis and osteoarthritis.
This guide will help you understand:
- where in the knee the condition develops
- how doctors diagnose the problem
- what treatment options are available
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Knee Pain|limit:15|heading:Hear from some of our patients who we treated for *Knee Pain*#
Anatomy
What part of the knee is affected?
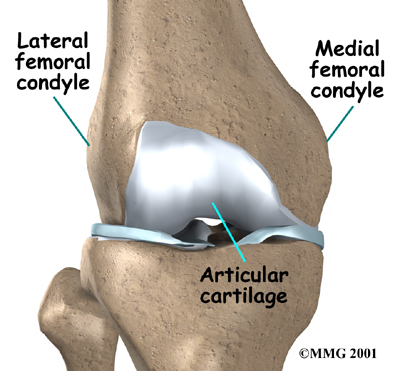
OCD mostly affects the femoral condyles of the knee. The femoral condyle is the rounded end of the lower thighbone, or femur. Each knee has two femoral condyles, referred to as the medial femoral condyle (on the inside of the knee) and the lateral femoral condyle (on the outside). Like most joint surfaces, the femoral condyles are covered in articular cartilage. Articular cartilage is a smooth, rubbery covering that allows the bones of a joint to slide smoothly against one another.
Femoral Condyles
The problem occurs where the cartilage of the knee attaches to the bone underneath. The area of bone just under the cartilage surface is injured, leading to damage to the blood vessels of the bone. Without blood flow, the area of damaged bone actually dies. This area of dead bone can be seen on an X-ray and is sometimes referred to as the:
Osteochondritis Lesion
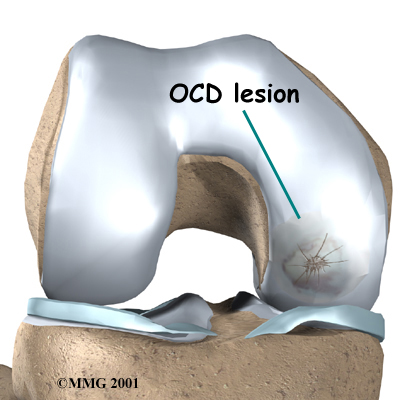
The lesions usually occur in the part of the joint that holds most of the body's weight. This means that the problem area is under constant stress and doesn't get time to heal. It also means that the lesions cause pain and problems when walking and putting weight on the knee. It is more common for the lesions to occur on the medial femoral condyle, because the inside of the knee bears more weight.
Related Document: Peak Performance Physical Therapy's Guide to Knee Anatomy
Causes
How does the condition develop?
Juvenile Osteochondritis Dissecans
Children as young as nine or ten can develop this condition. But the disease behaves much differently in children and for this reason is given a separate name, juvenile osteochondritis dissecans (JOCD), meaning osteochondritis dissecans of children.
OCD and JOCD cause the same kind of damage to the knee, but they are separate diseases. In the child who is still growing, the problem is much more likely to heal itself. In the adult, the bones are not growing. For this reason, the treatment and prognosis of OCD and JOCD can be very different.
Many doctors think that JOCD is caused by repeated stress to the bone. Most young people with JOCD have been involved in competitive sports since they were very young. A heavy schedule of training and competing can stress the femur in a way that leads to JOCD. In some cases, other muscle or bone problems can cause extra stress and contribute to JOCD.
Osteochondritis Dissecans
Sometimes JOCD is not treated or does not heal completely. When this happens, JOCD develops into OCD. OCD can occur any time from early adulthood on, but most patients are adults under age 50. The cases of OCD that are first diagnosed in early adulthood probably began as JOCD. When a person gets OCD later in life, it is probably a brand new problem.
Doctors aren't sure what causes OCD. There is less of a link between strenuous, repetitive use and OCD. Many people who develop OCD don't have any particular risk factors.
Because OCD leads to damage to the surface of the joint, the condition can lead to problems with bone degeneration and osteoarthritis. The damage to the joint surface affects the way that the joint works. Like a machine that is out of balance, over time this imbalance can lead to abnormal wear and tear on the joint. This is one cause of degenerative arthritis and osteoarthritis.
Related Document: Peak Performance Physical Therapy's Guide to Osteoarthritis of the Knee
Symptoms
What do OCD and JOCD feel like?
OCD and JOCD cause the same symptoms. The symptoms start out mild and grow worse with time. Both problems usually start with a mild aching pain. Moving the knee becomes painful, and it may be swollen and sore to the touch. Eventually, there is too much pain to put full weight on that knee. These symptoms are fairly common in athletes. They are similar to the symptoms of sprains, strains, and other knee problems.
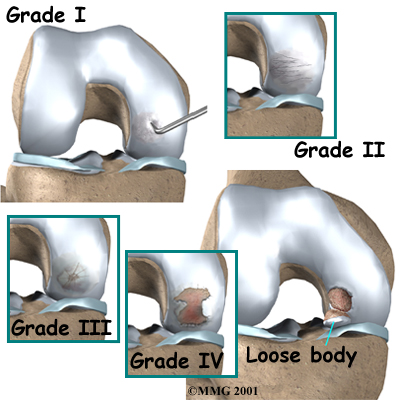
As the condition becomes worse, the area of bone that is affected may collapse, causing a notch to form in the smooth joint surface. The cartilage over this dead section of bone (the lesion) may become damaged. This can cause a snapping or catching feeling as the knee joint moves across the notched area. In some cases the dead area of bone may actually become detached from the rest of the femur, forming what is called a loose body. This loose body may float around inside of the knee joint. The knee may catch or lock when it is moved if the loose body gets in the way.
Diagnosis
When you visit Peak Performance Physical Therapy, our physical therapist will ask many questions about your medical history. We will ask about your current symptoms and about other knee or joint problems you have had in the past. Our physical therapist will then examine the painful knee by feeling it and moving it. You may be asked to walk, move, or stretch your knee. This may hurt, but it is important that we know exactly where and when your knee hurts.
Some patients may be referred to a doctor for further diagnosis. Once your diagnostic examination is complete, the physical therapists at Peak Performance Physical Therapy have treatment options that will help speed your recovery, so that you can more quickly return to your active lifestyle.
Our Treatment
How is this condition treated?
Many cases of JOCD can be completely healed with careful treatment. OCD will probably never completely heal, but it can be treated. There are two methods of treating JOCD: nonsurgical treatment to help the lesions heal, and surgery. Surgery is usually the only effective treatment for OCD.
Non-surgical Rehabilitation
Nonsurgical treatments help in about half the cases of JOCD. Our goals are to help the lesions heal before growth stops in the thighbone and to protect the injured area of cartilage while improving knee motion and strength. Even if imaging tests show that growth has already stopped, it is usually worth trying nonsurgical treatments. When these treatments work, the knee seems as good as new, and the JOCD doesn't seem to lead to arthritis.
Initially, it is crucial to stop doing everything that causes pain to the knee. This means stopping exercise and sports. It may require using crutches or wearing a cast for a couple of months when symptoms are present.
When you begin physical therapy at Peak Performance Physical Therapy, as knee symptoms ease, we can begin exercises that don't involve placing weight through your foot. The exercises will be done carefully and should not cause any pain. Our physical therapist may advise that you do exercises in a pool to help you stay limber and fit while protecting the knee during this period.
Range-of-motion and stretching exercises are used to improve knee motion. Our physical therapist may issue shock-absorbing shoe insoles to reduce impact and protect your knee joint. We will also show you strengthening exercises for the hip and knee to help steady the knee and give it additional protection from shock and stress.
Although the time required for recovery varies, nonsurgical treatment of JOCD can take from 10 to 18 months. Some patients who are too near the end of bone growth may not benefit with nonsurgical treatment. When these problems develop, our physical therapist may refer you for surgical evaluation.
Post-surgical Rehabilitation
If you have surgery, your surgeon may have you use a continuous passive motion (CPM) machine after surgery to help the knee begin to move and to alleviate joint stiffness.
With the exception of arthroscopic removal of a loose body, our physical therapists advise patients to avoid putting too much weight on their foot when standing or walking for up to six weeks. This gives the area time to heal. Weight bearing is usually restricted for up to four months after transplant procedures.
Patients are strongly advised to follow the recommendations about how much weight is safe. You may require a walker or pair of crutches for up to six weeks to avoid putting too much pressure on the joint when you are up and about.
After surgery, your first few physical therapy treatments are designed to help control the pain and swelling from the surgery. Our physical therapists will also work with you to make sure that you are only putting a safe amount of weight on the affected leg.
We choose exercises to help improve knee motion and to get the muscles toned and active again. At first, emphasis is placed on exercising the knee in positions and movements that don't strain the healing part of the cartilage. As the program evolves, our physical therapist will choose more challenging exercises to safely advance the knee's strength and function.
Ideally, patients will be able to resume their previous lifestyle activities. Some of our patients may be encouraged to modify their activity choices, especially if an allograft was used.
At Peak Performance Physical Therapy, our goal is to help you keep your pain under control, ensure safe weight bearing, and improve your strength and range of motion. When your recovery is well under way, regular visits to our office will end. Although we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
Peak Performance Physical Therapy provides services for physical therapy in Baton Rouge.
Surgery
If the lesion becomes totally or partially detached, surgery is needed to remove the loose body or to fix it in place. Your surgeon will need to gather lots of information about your knee and your problem before surgery.
This may require additional bone scans, X-rays, or MRIs. Your surgeon may also use an arthroscope, a tiny camera inserted into the knee to look at your knee before doing surgery to fix the problem. These tests are important because your surgeon needs to know the exact location and the size of the lesion to determine what kind of surgery will work best.
Arthroscopic Method
In some cases, your surgeon will be able to use the arthroscope to do the surgery. If the arthroscope can be used, the procedure requires smaller incisions than for an open surgery. This may reduce the time needed before the knee can be moved and exercised.
Open Method
Open surgery is needed when your surgeon can't get a picture of the entire lesion, when it is unclear how the fragment would best fit into the bone, or when it would be too difficult to replace the fragment using the arthroscope. Open surgery usually requires larger incisions than arthroscopic surgery to allow the surgeon to see into the knee and perform the operation.
Fragment Repair
If the loose bone fragment is in a weight-bearing area of your bone, your surgeon will try to reattach it if at all possible. Your surgeon may use tiny metal pins or screws to hold the fragment in place. This sometimes proves difficult. The damaged fragment often doesn't fit perfectly into the bone anymore. And the bone around the fragment has often changed in ways that mean your surgeon will need to rebuild it.
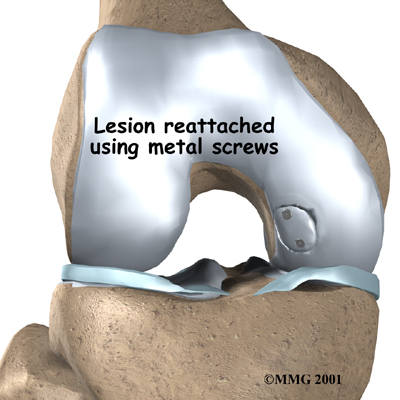
Despite the difficulties, reattaching the fragment generally results in much better knee function than removing it. Your knee will not be as good as new, but a careful plan of exercise and follow-up care can help you use your knee again without pain.
Allograft Transplant
In rare cases, the lesion must be removed from a weight-bearing area. Your surgeon may try to fill in the hole using an allograft. An allograft is an actual transplant of bone and cartilage from a donor into your knee. The bone is usually obtained from a bone and tissue bank.
In this case, bone material is transplanted into the hole left in the bone. Allografts have risks, including graft rejection and infection. But they can be very successful in returning function to the knee.
Osteochondral Autograft
An autograft is a procedure for grafting tissue from the patient's own body. The place where the graft is taken is called the donor site. In this case, surgeons graft a small amount of bone (osteo) and cartilage (chondral) from the donor site to put into the lesion. Usually, the donor site for this procedure is on the joint surface of the injured knee. Surgeons are careful to take the graft from a spot that won't cause a lot of problems, usually on the top and outside border of the knee cartilage. Even then, people sometimes end up with problems around the donor site. Surgeons have gotten good results with this surgery, but it is challenging to contour the graft to be just the same shape as the covering of the joint.
Autologous Chondrocyte Implantation
A new technology called autologous chondrocyte implantation is currently being developed. It involves using cartilage cells (chondrocytes) to help regenerate articular cartilage. This technology looks promising for treating JOCD and OCD but is still very much experimental.
Related Document: Peak Performance Physical Therapy's Guide to Articular Cartilage Problems of the Knee
Portions of this document copyright MMG, LLC.