Introduction
Physical therapy in Baton Rouge for Hand Issues
Welcome to Peak Performance Physical Therapy’s guide to endoscopic tunnel release. 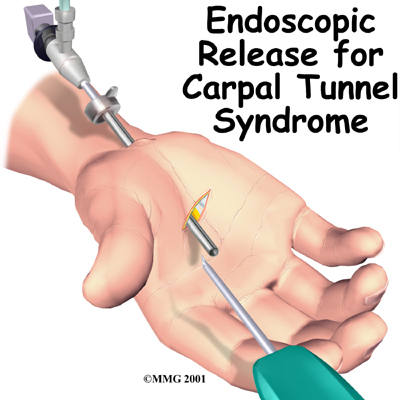 Carpal Tunnel Syndrome (CTS) is a condition affecting the wrist and hand. While the most common surgical procedure for carpal tunnel syndrome is still the open-incision technique, some surgeons are using a new procedure, called endoscopic carpal tunnel release.
Carpal Tunnel Syndrome (CTS) is a condition affecting the wrist and hand. While the most common surgical procedure for carpal tunnel syndrome is still the open-incision technique, some surgeons are using a new procedure, called endoscopic carpal tunnel release.
This procedure is done using an endoscope (a small, fiber-optic TV camera) to look into the carpal tunnel through a small incision just below the wrist. Using the camera allows the surgeon to release the problematic tissue without disturbing the overlying tissues.
This guide will help you understand:
- what part of the wrist is treated during surgery
- how surgeons perform the operation
- what to expect before and after the procedure
- what Peak Performance Physical Therapy’s approach to rehabilitation is
Anatomy
What part of the wrist is treated during surgery?
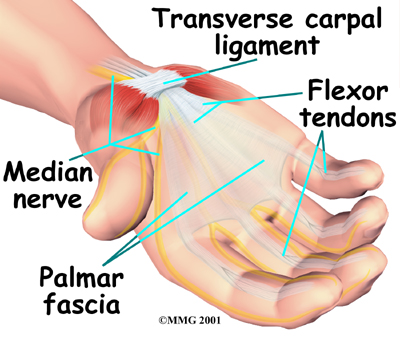
The carpal tunnel is an opening through the wrist into the hand that is formed by the bones of the wrist (carpal bones) on one side and a ligament, the transverse carpal ligament, on the other (ligaments connect bones together.) The transverse carpal ligament is at the base of the wrist and crosses from one side of the wrist to the other (transverse means across). It is sometimes referred to as the carpal ligament.
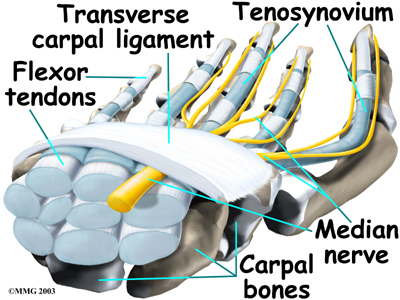
The median nerve, as well as the flexor tendons of the fingers pass through the carpal tunnel. The median nerve rests on top of the tendons, just below the carpal ligament. Between the skin and the carpal ligament is a thin sheet of connective tissue called the palmar fascia.
CTS is a common problem affecting the hand and wrist. Symptoms begin when the median nerve gets squeezed inside the carpal tunnel of the wrist, a medical condition known as nerve entrapment or compressive neuropathy. The carpal tunnel cannot expand so any condition that makes the area inside the carpal tunnel smaller or increases the size of the tissues within the tunnel can lead to symptoms of CTS. Any increase in pressure within the carpal tunnel can reduce blood flow to the median nerve, leading to symptoms and loss of nerve function.
Related Document: Peak Performance Physical Therapy's Guide to Hand Anatomy
Rationale
What does the surgeon hope to achieve?
Endoscopic carpal tunnel release surgery releases the carpal ligament, taking pressure off the median nerve. By using the endoscope, surgeons can accomplish this without disrupting the nearby tissues.
Proponents of the procedure feel that patients heal quicker than with an open surgery, are able to use their hand faster, and have fewer problems regarding tenderness of the palmar incision. Other physicians, however, are not convinced that this procedure for releasing the carpal ligament is better than the open-incision technique.
On the negative side, the endoscopic method is more technically demanding and can be more expensive in most hospitals. There may be a higher complication rate with this procedure involving incomplete release of the carpal ligament or injury to the median nerve inside the carpal tunnel. As more and more surgeons choose to use this method, these questions will likely be resolved.
Preparation
What should I do to prepare for surgery?
The decision to proceed with surgery must be made jointly by you and your surgeon. You need to understand as much about the procedure as possible. If you have concerns or questions, you should talk to your surgeon.
Once you decide on surgery, your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn't eat or drink anything after midnight the night before. This surgery can usually be done as an outpatient procedure, meaning that you can leave the hospital the same day.
Surgical Procedure
What happens during the operation?
The surgery is occasionally done using a general anesthetic (one that puts you to sleep). More often, however, a regional anesthetic is used. A regional anesthetic blocks the nerves going to only a portion of the body. Injection of medications similar to lidocaine are used to block the nerves for several hours. This type of anesthesia could be used for an axillary block (only the arm is asleep) or a wrist block (only the hand is asleep). The surgery can also be performed by simply injecting lidocaine around the area of the incision.
Once anesthesia is achieved, your surgeon will make sure the skin of your wrist area is free of infection by cleaning the skin with a germ-killing solution.
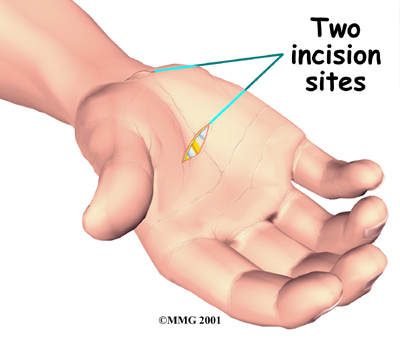
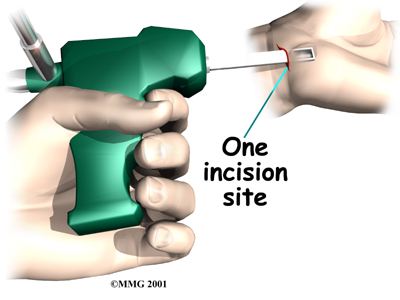
The surgeon nicks the skin to create a small opening just below the crease in the wrist where the palm starts. This opening allows the surgeon to place the endoscope into the carpal tunnel. Some surgeons make a second small incision within the palm of the hand, however the procedure using a single incision is becoming more popular. The incision allows the surgeon to open the carpal tunnel just below the carpal ligament.
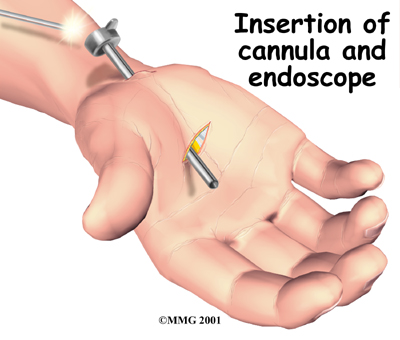
 Once the surgeon is sure that the instruments can be passed into the carpal tunnel, a metal or plastic cannula (a tube with a slot on the side) is placed alongside the median nerve. The endoscope can be placed into the tube to look at the underside of the carpal ligament, making sure that the nerves and arteries are safely out of the way.
Once the surgeon is sure that the instruments can be passed into the carpal tunnel, a metal or plastic cannula (a tube with a slot on the side) is placed alongside the median nerve. The endoscope can be placed into the tube to look at the underside of the carpal ligament, making sure that the nerves and arteries are safely out of the way.
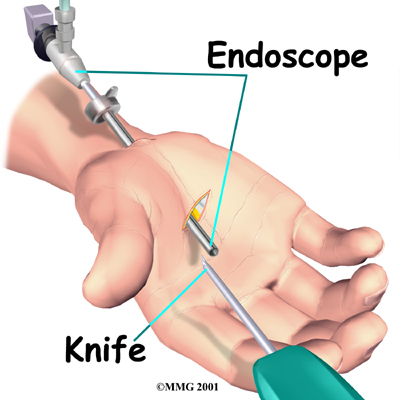
A special knife is inserted through the cannula. This knife has a hook on the end that cuts backwards when the knife is pulled back out of the cannula. Once the knife is pulled all the way back, the carpal ligament is divided, without cutting the palmar fascia or the skin of the palm.
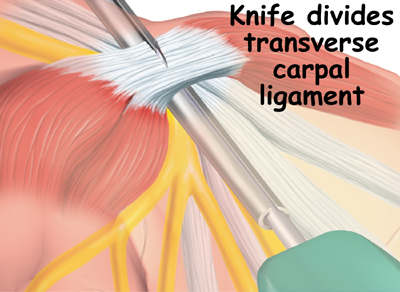
Once the carpal ligament is divided there is more space available in the carpal tunnel, which means the median nerve is no longer compressed.
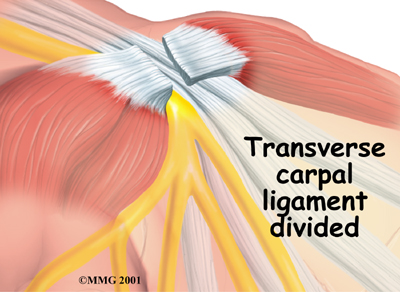
After the carpal ligament is released, the surgeon stitches just the skin openings and leaves the loose ends of the carpal ligament separated to keep pressure off the median nerve. Eventually, the gap between the two ends of the ligament fills in with scar tissue.
After Surgery
What happens immediately after surgery?
After surgery, the incision is wrapped in a soft dressing or simply covered with a bandage. Your surgeon may splint and wrap the wrist.
You'll be scheduled to see your doctor in 10 to 12 days for a follow-up. Your surgeon may need to take out one or two of the stitches if they haven't already been absorbed into your body.
Call your surgeon's office if you feel your hand is not healing as it should.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. This document doesn't provide a complete list of the possible complications, but it does highlight some of the most common problems, which are:
- anesthesia complications
- infection
- incision pain
- persistent symptoms
- incomplete ligament release
- hand weakness
Anesthesia
Problems can arise when the anesthesia given during surgery causes a reaction with other drugs the patient is taking. In rare cases, a patient may have problems with the anesthesia itself. In addition, anesthesia can affect lung function because the lungs don’t expand as well while a person is under anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Infection
Infection is a possible complication after surgery, especially infection of the incision. The warning signs of infection (or possibly other complications) are:
- pain in your hand that is not relieved by your medication
- discharge with an unpleasant odor coming from your incision
- swelling, heat, and redness along your incision
- chills or fever over 100.4 degrees Fahrenheit or 38 degree Celsius
- bright red blood coming from your incision
To monitor for an infection check your incision every day as instructed by your surgeon. If you think you have a fever monitor your temperature. If you have signs of infection or other complications, call your surgeon right away.
Incision Pain
Some patients report having pain along the palmar incision, but this complication occurs less than when people have an open release procedure. Sometimes people still feel some numbness and tingling after surgery, especially if they had severe pressure on the median nerve prior to surgery. If the thenar (thumb) muscles prior to surgery have notably shrunken (atrophied) from prolonged pressure on the median nerve, strength and sensation may not fully return even after having this type of surgery.
Persistent Symptoms
There is a small chance that problems of CTS don't go away completely. Sometimes symptoms come back after having the endoscopic release surgery. A return of symptoms is rare, but the likelihood is greatest in workers who go back to a job where they hold on to vibrating tools for long hours.
Incomplete Ligament Release
Releasing the carpal ligament using an endoscope requires skill and experience. One drawback of this procedure is incomplete release of the carpal ligament. When this occurs, symptoms may not go away completely. Some patients end up needing a second surgery to completely release the carpal ligament.
Hand Weakness
Muscles that are used to squeeze and grip may seem weak after surgery. During normal gripping, the tendons of the wrist press outward against the carpal ligament. This allows the carpal ligament to work like a pulley to improve grip strength. People used to think that the tendons lose this mechanical advantage after the carpal ligament has been released causing hand weakness. Recent studies, however, indicate that hand weakness is more likely from pain or swelling that occurs in the early weeks after the procedure rather than from lost mechanical advantage. With the exception of patients who have severe atrophy at the time of surgery, most people achieve normal hand strength within two to four months of surgery with the assistance of physical therapy. Those with severe atrophy commonly see improvements in hand strength, but they rarely regain normal size of the thenar muscles.
Rehabilitation
What should I expect after surgery?
Physical therapy at Peak Performance Physical Therapy will begin once your surgeon allows it. Often therapy can begin nearly immediately after your initial follow up visit with your surgeon. Even before that time your surgeon may have suggested you do some gentle finger motion exercises to start moving the tendons and tissues at the surgical site.
Your first few physical therapy sessions at Peak Performance Physical Therapy will focus on relieving the pain associated with the surgical procedure itself. Your therapist may use modalities such as heat, ice, ultrasound, or electrical current to assist with decreasing any pain or swelling you have around the surgical site or anywhere along the arm or into the hand. Massage to these areas may also be done in order to improve circulation and assist with the pain.
The next part of our treatment will focus on regaining the range of motion and strength in your wrist and hand, and if restricted also in your elbow, and shoulder. Your physical therapist at Peak Performance Physical Therapy will prescribe a series of range of motion and strengthening exercises that you will practice in the clinic and also learn to do as part of a home exercise program. If scar tissue builds up and impedes the motion of the tendons or nerves at the surgical site, similar symptoms to those you experienced before the surgery can occur. For this reason your therapist will teach you special range of motion exercises for your hand, wrist, elbow and shoulder that help to glide the tendons and nerves of the wrist through the surgical site.
Strengthening exercises may include the use of rehabilitation equipment such as putty, elastics, as well as small weights or balls in order to add strengthening and gripping resistance. Strengthening of the muscles that bend your wrist up as well as those that move the thumb will be specifically focused on since these muscles are supplied by the median nerve so they may have specifically lost strength due to the CTS. Most light exercises can be started fairly quickly but heavy grasping or pinching will not be encouraged until about 6 weeks post surgery in order to avoid the tendons pushing out against the healing carpal ligament. In addition to strengthening your wrist muscles and grip strength we will educate you on ways to hold items and use your wrist and hand such that you don’t put unnecessary stress on your healing tissues and to avoid any future pain.
If necessary, your physical therapist will mobilize the joints of your wrist or hand if they are particularly stiff after the surgery. This hands-on technique encourages the stiff joints to move gradually back into their normal range of motion.
Being able to use your wrist fully so that you can complete your work tasks and daily activities is the goal of our therapy at Peak Performance Physical Therapy. Maximizing dexterity and fine motor control of the hand can greatly improve the functional use of your hand and wrist. For this reason, as part of your rehabilitation we will also include activities such as picking up items from a table, twisting items into place, or doing tasks with your hand that are similar to your regular work or sporting activities. These functional activities encourage the joints and the muscles of the hand and wrist to work in unison, which is critical to maximizing the use of your entire upper limb.
A final, but extremely important part of our treatment for you at Peak Performance Physical Therapy following endoscopic carpal tunnel release is to discuss your overall posture and alignment. Pressure in your wrist can stem not only from direct pressure at the wrist but also from compensatory posturing patterns that start even as high up as the neck! If you are required to sit for long periods at the computer you can easily develop poor posture which puts pressure on the nerves that run from the neck through the shoulder and elbow, and down into the wrist and hand. Poor elbow or wrist posturing as they rest on your chair or desk can also heavily contribute to an injury in the area. Desk workers, however, are not the only sufferers from poor posturing. Anyone can be affected the same way if their posture is poor over a long period of time. Correcting your posturing and doing exercises to strengthen the muscles that help to keep you in a proper posture position is crucial in avoiding further symptoms in the future. Your physical therapist will advise you on proper posturing while standing, sitting, and during other functional tasks, and if you are an office worker, they can also help you to adjust your workstation to ensure there is the least amount of strain on your body as possible.
When you are well underway, regular visits to Peak Performance Physical Therapy will end. Your therapist will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program.
In the majority of cases the physical therapy we provide at Peak Performance Physical Therapy after endoscopic carpal tunnel release surgery occurs without any complications. If, however, during rehabilitation your pain continues longer than it should or therapy is not progressing as your physical therapist would expect, we will ask you to follow-up with your surgeon to confirm that your wrist is tolerating the rehabilitation well and to ensure that there are no complications that may be impeding your recovery.
Portions of this document copyright MMG, LLC.
Peak Performance Physical Therapy provides services for physical therapy in Baton Rouge.